Obamacare vs. Omamacare Don't throw Mama off the dialysis machine
You can look at this story as a continuation of "Don't Throw Mama off the Turnpike." That's when she and I caravan my 2002 "Free State Audi" with her 1997 Mercury Villager into the middle of New York State for the purpose of selling said Audi to an unlikely buyer.
Roughly 10 days ago, Mama Bear went in for a checkup with the kidney doctor.[1] Whoops! Blood pressure is far too high, other symptoms conclusive of renal failure. [Now I'm kicking myself for pressing her into duty as my "wing man" on the long-range, grueling trip to make the Audi transaction. Has she blown a gasket because of my callous insensitivity?] To make a long story short, she needs to undergo dialysis, a process where an external kidney machine performs the filtration of metabolic wastes from the blood.
Informing the health care debate...
It occurred to me to share at least the initial few days of the activities that Mom (83) and I (60) perform getting her plugged into the lifesaving technology that, today, has become routine.
Approximately 300,000 people in the United States are on dialysis, which seems to have the most prevalence of any country by far. In Mom's case, she has no other health issues, so it's likely this blood-cleanup operation will significantly improve her quality of life... in return for three sessions a week approximately three hours per session. [Per Dr. Kidney Guy, it's possible, even hopeful, the full regimen won't be necessary indefinitely.]
Anyway, let's use Mom's experience as an instance of how the health system works now in the case of a significant medical problem for a real person of a certain socioeconomic class in America. "Omamacare: If it's broke, what's to fix?" Mom entered the work force independently in the 1970s as a highschool teacher, then law school administrator, then college teacher, finally a life and casualty insurance wonk for a big firm in Texas. Through due diligence, she acquired a couple of modest pensions, which, along with Social Security, give her a better income situation than most widows her age. But aside from me there's no one to really look after her.
Another factoid in the Omamacare equation: when Mom became 65 she hooked up with a supplemental Medicare health-insurance program available through Henry Ford Health Care Systems called Health Alliance Plan. Not to sound like an advertisement, but the HAP connection proved to be super good fortune: for a relative pittance of ~$50 a month, she's covered for, like, everything... from CAT-scans to eye operations to, well, kidney failure. And, unlike the horror stories of Michael Moore's Sicko, where state-enabled corporate sadists routinely violate insurance contracts with impunity, HAP is totally straight up.
So maybe Mom is a lucky one to have finessed the current system. Or maybe the HAP approach provides a health-care architecture kernel for a genuine low-cost, high-quality, fully voluntary market system of universal health care. All I know is if Obamacare kills Mom's HAP-based Omamacare, her quality and quantity of life will be majorly stuffed. Even with Omamacare—as we'll see directly—the amount of government is plenty scary.
Hooking up the drain and fill ports
Dialysis requires that the patient's blood be circulated through a sophisticated filtration system continuously for hours at a time. Typically (initially) patients are fitted with a catheter system that inserts a dual-channeled conduit into a major blood vessel. A portion of the bloodflow is drawn through the input side of the conduit, then
returned through the output channel of the conduit back into the patient's circulation. The first step is to hook Mama up with this catheter, so she won't need to get poked with needles (and risk arrest as a drug addict) every dialysis session.
Destination Henry Ford West Bloomfield, a place they call radiological intervention.
Here, I'm not so much attending to the medical procedure as to the new wing of the facility—it looks like something out of Star Trek: the Feng Shui episode. With a full-service cafeteria, coffee shops, gift shops, open air sidewalk cafes, and a cardiology center that resembles the lobby of the Hyatt Regency, the new Henry Ford West Bloomfield is leading edge in esthetics. However, someone needs to go out and round up some customers. There's no one here. Maybe it's the hour.
Everything goes smoothly, and why would it not. We're out here in the burbs in these state-of-the-art—and, it would appear, underutilized— facilities; plus it's covered. After we learn how to spell and pronounce "interventionist radiology," we find the chambers where the "interventionist radiologist" splices the catheter into one of Mom's big vessels. Kind of a drag, as the procedure (performed under local anesthetic) takes 45 minutes, then she has to sit around for two hours to make sure nothing springs a leak I guess. They have Wifi, so I use the time to do some work writing shopping cart
software reviews... and I wander around the prow of the spaceship.
Onward to the Tidy-Blood Center...
This first part of our contact with the health care system has been generally positive. The clerical and medical staff have been informative, helpful, and pleasant. You might think that the care standards are higher out here in the burbs because there's a relatively high percentage of care givers to care needers. But, when Mom had the eye problem, I took her down to the main, original Henry Ford Hospital in Detroit proper. That location was relatively dense with care needers, most obviously with minimal material means. I recall that even there, the hospital did pretty well in moving people along efficiently and dispensing quality attention.
Mom's situation is more urgent than most. Ordinarily, when dialysis has been prescribed, the patient has some orientation classes and time to make decisions on the methods. But no sooner has the anesthetic worn off we get the word from Dr. Kidney Guy's people that we're set up for initial dialysis two days from now. On the day, we travel directly eastbound from the Novi homestead about 10 miles, where the designated dialysis facility lies... let's call it the Tidy-Blood Center (TBC).
Well, this step points out some flies in the ointment of the Omamacare system... at least when it comes to wholistic kidney treatment in a major metropolitan area. The first quake of anxiety hits me when I see someone has set a bunch of Triffids (large man-eating plants) on all the flat surfaces where one normally signs in. Oh oh. There's an extremely large black woman[2] obscured behind the plants who apparently has the job of getting our paperwork in order. We hand clipboards back and forth through the petals and leaves. Good thing I'm here, because Mom is only 5'4" and wouldn't have seen anyone back there behind the counter.
Who's in charge here? Does anyone introduce themselves, extending a welcome to Mom or to me, letting us know what's going on? No. Large #1 is nice but let's just say unswift. Plus, she's clearly a drone bee. Next, Large #1's boss(?)/replacement(?) shows up and seems to be taking charge. This woman has a 'tude. We've filled out and signed a few papers, nothing complicated, nothing that should take more than 15 minutes, tops. But it's been 45 minutes that we've been sitting in a cramped waiting room, watching a parade of dialysis-needers file through... some waiting to be picked up and deposited in front of us.
I go to this new one—also off the charts on the weight scales[3]—saying something classy like, "So are we making progress? Any idea how much longer we'll be doing paperwork?" [I admit my anxiety level and, thus, anger level is rising. So I don't include the proper amount of respectful tones and sweet-nothings in my question.] She senses the hostility, and mutters something under her breath, sounds like, "Guess you be done when I say, boy."
Message understood, I back off.
Mama Bear, bless her little pea-pickin' heart, has become resigned to whatever the fats—er, I mean the fates—have in store. But my head is swimming now in confusion. There are too many relationships: there's the coordinator Judy who supposedly sets up the dialysis program, there's a Jane and an Anne who are administrators for Dr. Kidney Guy at the clinic, there was someone else I spoke with in radiology, there's the doctor himself, there are these two asteroidal bodies in front of me, then patients walking or rolling by seemingly randomly, and some apparent-staff people selling popcorn over in the corner.[4]
I can't figure it out at all. And it's making me agitated. Normally, I'm an easygoing guy, but these people are acting like my mom doesn't count. I'm about to start dialing phone numbers; first I take one more crack at Large #2. "Listen, can you tell me what's going on? Who's responsible for taking care of Phyllis Wright, is that you? Or do I call the doctor, or the coordinator, or the washroom attendant." I don't really remember what I said, but it could definitely have come off as smart-ass. Maybe she gets the idea I'm not going to back down again, or maybe she senses I'm Potential Crazy Man with an AK-47 in the car, but she quickly passes me to the social worker—they have two—let's call her Helga.
Helga is the drink of water I need. She's "white-like-me,"[5] statuesque, attractive and calming. We're going to meet and chat. First, Mom has cleared her incomprehensibly long paperwork hurdles, and I accompany her to the room where all the dialysis stations are laid out. The technicians back there have practical body dimensions and seem to know what the flock they're doing. Now we're making progress.
Hello, Mom. She's in the pod closest to us on the right.
As I say, the entry process into the TBC has been less than wonderful. But truthfully, the only negatives have to do with the two-body bottleneck at the front counter, which had assumed an authority way out of proportion to their psychological reality. This interaction with personnel at the TBC reminds me of dealing with a rather specific set of people I've run into before in the metro-corporate world. [Out of scope of the current discussion.]
Let's just call the general phenomenon: Incompetent Hostile Authority (IHA) Syndrome. At least, here with Omamacare, competent staff seems to know how to work around speed-bump staff.
With Obamacare—which, regardless of how one sugarcoats it, amounts to a massive governmentalization of the healthcare business—the number of IHAs (black, white, male, female) will grow substantially. [Government is authority, coercive authority.] Far faster than competent staff can overcome or remove the damage. Further, IHAs will come into more authority, including medical authority, e.g. government systems like the homicidal FDA already. Health care will not only suffer, hospitals will become glorified killing fields... though if you're fortunate to live in West Bloomfield you'll draw a high triage number, then go out in style.
I'd love some comments or posts on the Coffee Coaster Blog regarding health care. From my perspective, Omamacare
is a solid foundation. When you're experiencing the system you realize that these are people delivering the care. If it's a business—even a nonprofit one (which, IMHO, has a lot to recommend it)—you as a care worker have natural incentives to provide the best care at the lowest cost. No such incentives exist in government systems, indeed, quite the opposite. By and large, the people in Omamacare have been wonderful.
How would one democratize Omamacare? Well, start by enabling people of all ages to acquire Health Alliance Plan-type insurance, while at the same time removing government-corporate privilege, compulsion, and prohibition from the system. Decorporatize health care, or at least open health care to unfettered nonprofits and charitable-giving operations. Prices for healthcare decline, alternatives increase. One final thought: it would be fabulous if every health care needer had an individual advocate... kind of like an agent. And I'm busy.
Whatever we do, we mustn't throw Mama off the dialysis machine.
###
[1] Mom has a condition known as polycystic kidneys, which cysts accumulate in the kidney tissue and cause the kidneys to reduce function (her's is ~7%). It's hereditary. The childhood version is fatal.
[2] When I say extremely large, I mean obese to the point of tragedy... 500 pounds if she's an ounce.
I doubt her fingertip could punch a single key by itself on a keyboard, she can barely turn around inside her cubicle area, her breathing and her speech are labored, I'm worried she'll simply petrify in place.
[3] Think about the situation though. Mom is assigned to a facility for life-saving, health-giving treatment, which facility's public interface consists of two women who physically have a hard time lifting a finger. What kind of message does that send to children?
[4] Not really selling popcorn, rather giving away sandwiches and snacks to the several patient-clients
leaving. It's the end of the month, and as I eventually figure out, the staff and the patient-clients come to feel like a family.
[5] I'd be lying if I said I didn't feel any anti-white antagonism from Large #2 and a couple of the other black women in the facility. Even when I'd ask a simple, polite (post-procedural) question of these individuals, it's as if I were a county-jail inmate asking about my accommodations. Large #2 and the black social worker seemed to think I was stupid for requesting a written schedule of Mom's appointed dialysis times.
"Can't you understand 10:30 Mondays, Wednesdays, and Fridays?" Black social worker then repeats the schedule real slow and more loudly.



 You can look at this story as a continuation of "
You can look at this story as a continuation of "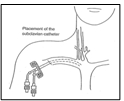 Dialysis requires that the patient's blood be circulated through a sophisticated filtration system continuously for hours at a time. Typically (initially) patients are fitted with a catheter system that inserts a dual-channeled conduit into a major blood vessel. A portion of the bloodflow is drawn through the input side of the conduit, then
returned through the output channel of the conduit back into the patient's circulation. The first step is to hook Mama up with this catheter, so she won't need to get poked with needles (and risk arrest as a drug addict) every dialysis session.
Dialysis requires that the patient's blood be circulated through a sophisticated filtration system continuously for hours at a time. Typically (initially) patients are fitted with a catheter system that inserts a dual-channeled conduit into a major blood vessel. A portion of the bloodflow is drawn through the input side of the conduit, then
returned through the output channel of the conduit back into the patient's circulation. The first step is to hook Mama up with this catheter, so she won't need to get poked with needles (and risk arrest as a drug addict) every dialysis session.
 Destination Henry Ford West Bloomfield, a place they call radiological intervention.
Here, I'm not so much attending to the medical procedure as to the new wing of the facility—it looks like something out of Star Trek: the Feng Shui episode. With a full-service cafeteria, coffee shops, gift shops, open air sidewalk cafes, and a cardiology center that resembles the lobby of the Hyatt Regency, the new Henry Ford West Bloomfield is leading edge in esthetics. However, someone needs to go out and round up some customers. There's no one here. Maybe it's the hour.
Destination Henry Ford West Bloomfield, a place they call radiological intervention.
Here, I'm not so much attending to the medical procedure as to the new wing of the facility—it looks like something out of Star Trek: the Feng Shui episode. With a full-service cafeteria, coffee shops, gift shops, open air sidewalk cafes, and a cardiology center that resembles the lobby of the Hyatt Regency, the new Henry Ford West Bloomfield is leading edge in esthetics. However, someone needs to go out and round up some customers. There's no one here. Maybe it's the hour.
 "interventionist radiology," we find the chambers where the "interventionist radiologist" splices the catheter into one of Mom's big vessels. Kind of a drag, as the procedure (performed under local anesthetic) takes 45 minutes, then she has to sit around for two hours to make sure nothing springs a leak I guess. They have Wifi, so I use the time to do some work writing shopping cart
"interventionist radiology," we find the chambers where the "interventionist radiologist" splices the catheter into one of Mom's big vessels. Kind of a drag, as the procedure (performed under local anesthetic) takes 45 minutes, then she has to sit around for two hours to make sure nothing springs a leak I guess. They have Wifi, so I use the time to do some work writing shopping cart  Well, this step points out some flies in the ointment of the Omamacare system... at least when it comes to wholistic kidney treatment in a major metropolitan area. The first quake of anxiety hits me when I see someone has set a bunch of
Well, this step points out some flies in the ointment of the Omamacare system... at least when it comes to wholistic kidney treatment in a major metropolitan area. The first quake of anxiety hits me when I see someone has set a bunch of 
 With Obamacare—which, regardless of how one sugarcoats it, amounts to a massive governmentalization of the healthcare business—the number of IHAs (black, white, male, female) will grow substantially. [Government is authority, coercive authority.] Far faster than competent staff can overcome or remove the damage. Further, IHAs will come into more authority, including medical authority, e.g.
With Obamacare—which, regardless of how one sugarcoats it, amounts to a massive governmentalization of the healthcare business—the number of IHAs (black, white, male, female) will grow substantially. [Government is authority, coercive authority.] Far faster than competent staff can overcome or remove the damage. Further, IHAs will come into more authority, including medical authority, e.g.